Across Africa, women are often the first point of contact in healthcare, serving as community health workers, nurses, caregivers, and public health practitioners. Yet when critical decisions about health systems are made, women remain significantly underrepresented in leadership. This disconnect has consequences. When the people closest to community realities are missing from decision-making tables, health programmes risk overlooking important perspectives that influence trust, access, and effectiveness.
Women make up 70% of the health workforce, yet they hold just 25% of senior roles. This leadership gap directly weakens public health. When women are underrepresented in leadership, programs often miss important perspectives on the needs of women, children, and local communities. Decision-making becomes less inclusive, community trust becomes harder to build, and health interventions tend to be less effective and responsive.
However, eHealth Africa (eHA) is actively changing this narrative. At eHealth Africa, inclusion is treated as a strategic investment rather than a standalone initiative. The organisation has intentionally created pathways that help women enter, grow, and lead across technical, operational, and leadership roles.
These pathways include gender-conscious recruitment practices, leadership development opportunities, mentorship programmes, flexible work arrangements, and family-friendly policies designed to support long-term career growth.
One of the women who has experienced this growth firsthand is Fozia Ahmad Malik, Director of People & Operations at eHealth Africa.
Her journey illustrates how intentional investment in talent can create leadership opportunities for women while strengthening organisational capacity. She joined eHA in 2018 as a Finance Manager. Through targeted support and clear pathways, she climbed to Senior Manager, transitioned to lead Grants Management, became Deputy Director, and today leads our entire People & Operations directorate as the Director.
Looking back on her experience, Fozia attributes much of her growth to a workplace culture that prioritises inclusion and professional development. She says, “From day one, I’ve felt a deep culture of respect and inclusion. Even as a brown woman working in another country, I’ve always felt seen, supported, and treated equally. That’s why I’m especially grateful for my journey at eHealth Africa.” She also highlights how practical support enables women to sustain their careers, noting that flexible work arrangements have been a game-changer because they create space for women to juggle their many responsibilities without guilt.

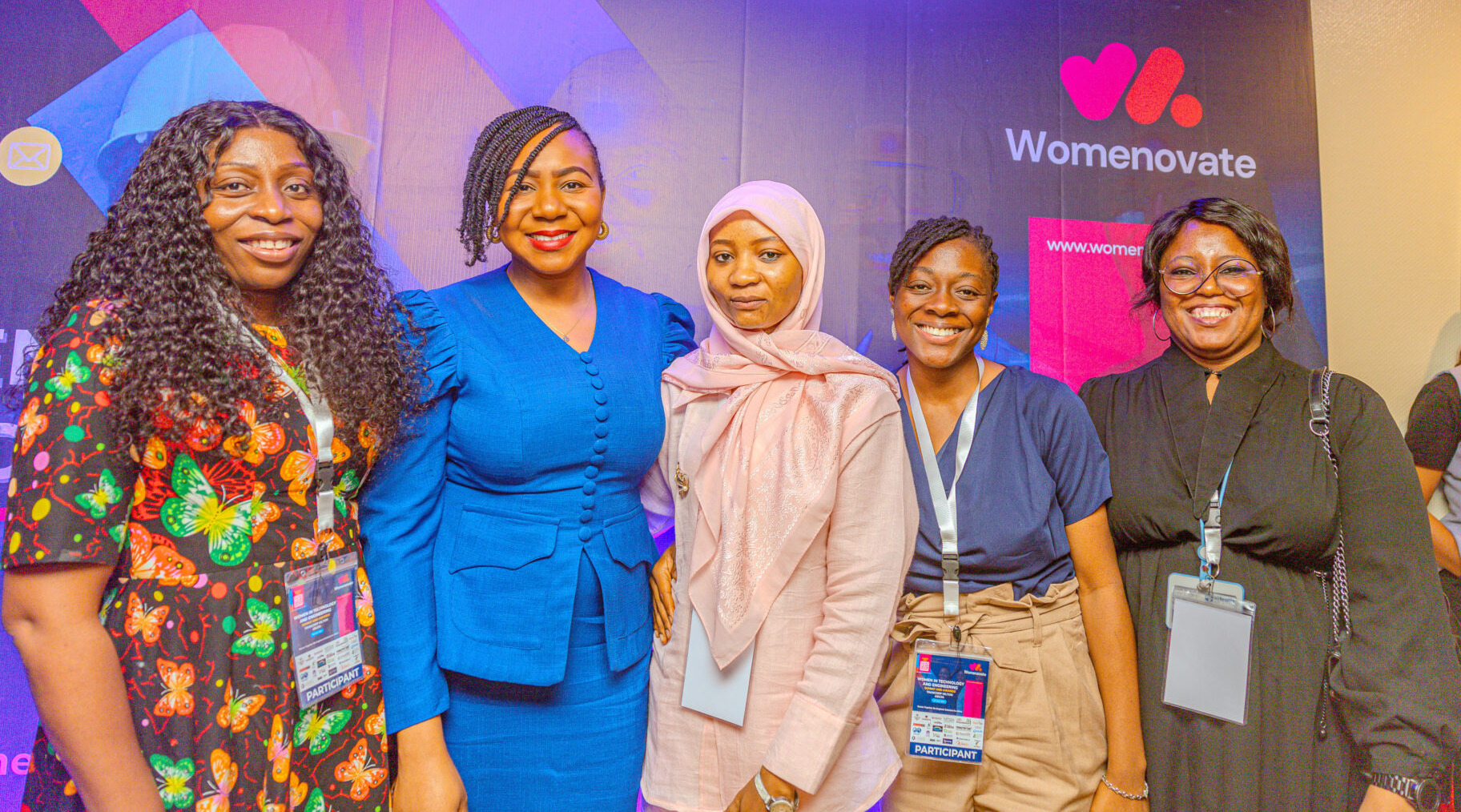
These intentional efforts are translating into measurable progress. Women currently represent 33.3% of eHealth Africa’s workforce and 34.7% of leadership positions, demonstrating that women are advancing into decision-making roles at a rate that exceeds their overall workforce representation. Beyond the numbers, women who grow within the organisation tend to stay longer, take on greater responsibilities, and bring valuable insights that improve the quality of the organisation’s work.
For eHealth Africa, increasing women’s representation in leadership is not simply about workplace equity. Diverse leadership teams bring broader perspectives to programme design, community engagement, and operational decision-making. These perspectives help ensure that health interventions are better aligned with the realities of the communities they serve, particularly in areas such as maternal health, nutrition, immunisation, and community-based health programmes.
eHealth Africa continues to invest in inclusive initiatives, expanding mentorship and opportunities for women, using data to guide improvements, and creating an environment where women can thrive in leadership. Real and lasting progress will require collective commitment across governments, NGOs, and the private sector to dismantle structural barriers and outdated cultural norms.
At eHealth Africa, investing in women leaders is central to our mission. By empowering women to rise and lead, we build stronger, more resilient teams that deliver better health outcomes and create a deeper impact for the communities we serve. Building stronger health systems requires more than technology, funding, or infrastructure. It also requires leadership that reflects the communities those systems serve. By investing in women’s growth and leadership today, eHealth Africa is helping build a more inclusive, resilient, and responsive public health future across Africa.