It is August 2023, in a remote Nigerian village in Northern Nigeria. Children 5 years and below are on a queue waiting to be vaccinated against polio. At Least, 2,509,687 children have already benefited from the 18-day mass vaccination campaign to boost their immunity against Circulating Variant Poliovirus (cVPV2). (World Health Organization [WHO], 2023).
This raises an important question. If Nigeria was declared polio free in 2020, why do we still require polio vaccinations campaigns today? After years of collaborative efforts, significant progress was made in eliminating polio. However, the threat of circulating variant poliovirus (cVPV2) lingers, particularly in remote areas of Northern Nigeria. Efforts are being made to ensure that we see the end of this disease.
As Nigeria continues the journey towards finally eradicating polio, digital innovation has become a vital tool in ensuring the success of the country’s vaccination efforts. One of such innovative solutions is the integration of GIS tracking systems on eHealth Africa’s polio interventions. This revolutionary innovation has transformed how vaccination campaigns are planned, tracked, and executed.






Here are five key reasons why digital innovation is the game-changer in Nigeria’s final push to end polio.
1. Every community is reached with accuracy
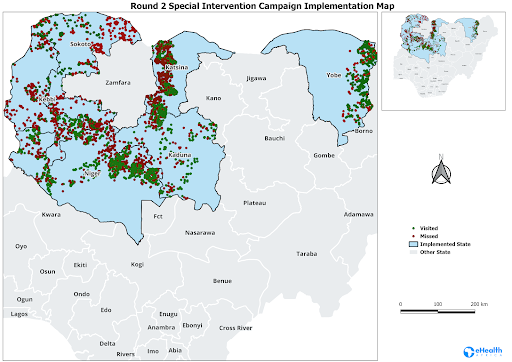
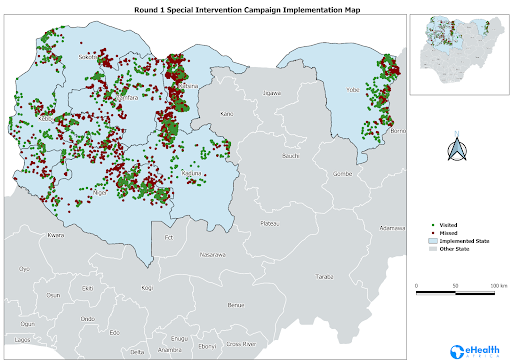
The foremost challenge in eradicating polio in Nigeria has been reaching remote and conflict-ridden areas where vaccination coverage is inconsistent. With difficult terrains, and insecurity, It is often nearly impossible to ensure that no child is left behind. With eHealth Africa’s GIS technology, teams are able to track and locate settlements in hard-to-reach areas with geo-coordinates of over 70% of settlements that were previously unmapped. This level of precision has allowed vaccination teams to better plan and ensure that no community is overlooked, increasing vaccination coverage rates. In 2023, the geo-coverage rate of vaccination activities tracked rose to 89%, representing a 6% increase over the previous quarter. This data-driven approach has been instrumental in reaching more than 1.4 million children in tracked settlements across the country.
2. Vaccination Campaigns are Monitored Real-time
One useful aspect of digital technology is its ability to provide real-time data and feedback. Vaccination campaigns can now be tracked in real time, allowing for immediate course corrections if any gaps are identified. The GIS technology has made it possible to track vaccination teams as they move from one settlement to another, providing health authorities with the data they need to ensure that every planned area is covered. With this technology during the vaccination campaign in April 2023 12,791 settlements across 56 LGAs in Katsina, Niger, Sokoto, and Zamfara, were reached, achieving an impressive 81% of the planned coverage. This real-time accountability has ensured that vaccine wastage is minimized, resources are optimally allocated, and the campaign’s impact is maximized.
3. Tailored Trainings for Vaccination Teams
Digital innovation not only improves logistical planning and monitoring but also equips health workers with the necessary tools and knowledge to enhance their effectiveness. With the GIS Intervention, eHealth Africa trained 107 individuals across five states—Katsina, Zamfara, Kebbi, Niger, and Sokoto—to effectively use digital tools and geospatial data to improve their vaccination outreach. These training efforts have empowered local teams and equipped health workers with the knowledge needed to adjust strategies on the go, to achieve more successful campaign outcomes.
4. Enhanced Micro Planning for Campaigns
Polio eradication requires meticulous planning, especially in regions where settlements are small, scattered, and often unmapped. Digital health tools have drastically improved micro planning by providing vaccination teams with up-to-date settlement data and templates to develop detailed vaccination plans. The Master List of Settlements (MLoS), regularly updated through digital tracking, serves as a comprehensive guide for teams in the field. This detailed approach has proven instrumental in increasing vaccination coverage in previously underserved areas, as seen in the 89% overall coverage rate achieved during the 2023 campaign, which targeted 4,861 settlements.
5. An Expandable Model for other Public Health Campaigns
The success of eHealth Africa’s GIS technology in Nigeria is proof that digital innovations can effectively address a wide range of other public health challenges. The systems, data infrastructure, and training models developed for polio eradication are not only efficient but also highly adaptable and can be applied to combat other diseases and public health emergencies.
The successful deployment of GIS technology by eHealth Africa in Nigeria is evidence that digital innovations can help in the solution of many other public health problems. The systems, data infrastructure, and training models developed for the polio eradication program are not only effective but also flexible enough to be used for other diseases and public health threats.
Through continued investment in these technologies, Nigeria is not only positioned to become polio-free but also to build a more robust and resilient healthcare system that will benefit generations to come.