Case Studies
Building Real-Time Public Health Command Centers for Mass Campaign Operations in Nigeria

Large-scale public health campaigns often operate in some of the most logistically challenging environments in the world. Across multiple states in Nigeria, field teams travel through remote settlements, areas with weak network connectivity, and locations affected by security constraints, all while attempting to deliver time-sensitive interventions and collect high-quality data (WHO, 2020). In these contexts, delayed reporting systems and fragmented supervision structures can significantly reduce operational effectiveness.
As public health programs increasingly adopt digital tools for implementation, the question is no longer whether data can be collected digitally, but whether that data can drive real-time operational decision-making (Mehl & Labrique, 2014). As an implementing partner providing data management and technical support for large-scale public health initiatives, eHealth Africa implemented a command center model that transformed field data collection into a coordinated operational intelligence system. The approach integrated near-real-time monitoring, centralized validation, GIS-enabled oversight, and rapid-response decision-making mechanisms to strengthen implementation quality across mortality assessments, census activities, and coverage evaluation surveys across multiple states in Nigeria.
The Operational Intelligence Architecture
The command center served as a centralized coordination hub, monitoring field data submissions, validating incoming data, identifying operational anomalies, and facilitating rapid issue resolution. Rather than relying solely on end-of-day reporting, dashboards connected to KoboToolbox APIs enabled near real-time visibility into field activities. This allowed teams to monitor submission trends, identify geographic gaps, and escalate data quality concerns during implementation rather than after project completion.
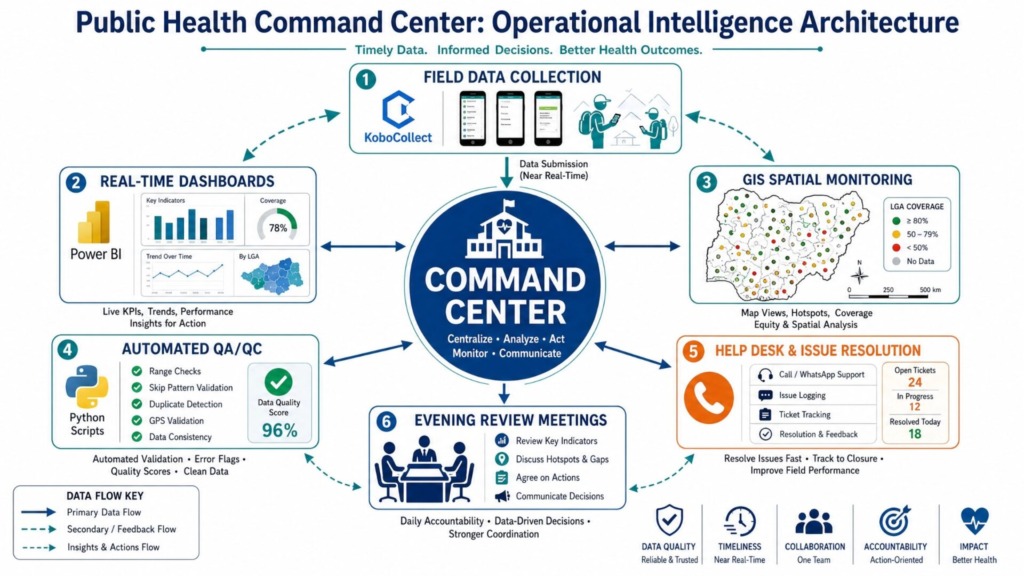
Figure 1: The operational intelligence architecture of the Public Health Command Center, illustrating the continuous flow of data from field collection to real-time decision making.
This operational model became particularly valuable during large-scale field deployments. Coordinating supervision at that scale required layered oversight systems. In Kaduna State, during the household enumeration, 5,268 enumerators were deployed, with a daily target of 150 households per enumerator. To manage this massive workforce, the supervision hierarchy included 255 Ward Focal Persons (WFPs) responsible for supervising and validating data collected at the ward level, and 3 LGA Coordinators per LGA (totaling 69 LGA Coordinators). At the apex of this structure, 50 data validators operated from the Command Center to validate real-time data. The command center structure provided a unified operational environment where field progress, validation outputs, and implementation challenges could be reviewed collectively and acted upon rapidly.
Evening Review Meetings: The Engine of Adaptive Management
One of the key operational innovations was the institutionalization of structured Evening Review Meetings (ERMs). These daily sessions served as operational feedback loops, bringing together supervisors, data validators, program teams, and project leads to review field performance, resolve technical challenges, and guide next-day implementation priorities.
Across multiple states, these meetings significantly improved coordination, strengthened accountability, and enabled adaptive planning during active implementation. LGAs with low coverage or significant data errors were publicly reviewed during these sessions, ensuring that underperformance was immediately addressed and corrective actions were agreed upon collaboratively.
Automated Quality Assurance at Scale
The command center approach also strengthened data quality assurance mechanisms. Automated validation pipelines integrated with Kobo APIs enabled rapid detection of:
- Duplicate household entries
- Stacked or falsified GPS coordinates
- Inconsistent household composition data
- Implausible survey durations
- Logical inconsistencies within forms
These systems reduced the turnaround time between data submission and corrective action, minimizing the accumulation of unresolved data quality issues. This rigorous approach results in a final dataset with zero duplicate households and a 100% data approval rate at the end of every implementation activity, before teams leave the field.
Geospatial Intelligence and Remote Verification
Importantly, the value of the command center extended beyond monitoring alone. The integration of GIS-enabled dashboards and geospatial intelligence transformed supervision into a more evidence-driven process.
In Kano State, geotracking systems enabled near real-time visualization of field movement patterns, settlement coverage, and implementation completeness during Mass Drug Administration (MDA) activities. Supervisors could identify missed settlements, assess geographic coverage gaps, and redeploy teams strategically based on live operational intelligence rather than retrospective reports. This remote verification capability was particularly crucial in security-compromised areas where physical supervision was unsafe.
Conclusion
This model represents an important shift in how public health campaigns are managed in resource-constrained settings. Traditional monitoring systems often emphasize retrospective reporting, where problems are discovered after implementation has ended. In contrast, command center operations support adaptive implementation, a model where programs continuously learn, adjust, and improve during active delivery (The Lancet Global Health, 2021).
As public health systems increasingly adopt digital implementation models, command centers can serve as critical infrastructure for strengthening operational efficiency, accountability, data integrity, and equitable service delivery. Their value is especially significant in large-scale campaigns where timely decisions can directly influence coverage quality and implementation outcomes.
Our experience demonstrates that command centers are no longer simply administrative support units. They are operational intelligence systems capable of transforming how complex public health interventions are monitored, coordinated, and optimized in real time.
References
- World Health Organization. (2020). Digital health interventions for health system strengthening. Geneva: WHO.
- Mehl, G., & Labrique, A. (2014). Prioritizing integrated mHealth strategies for universal health coverage. Science, 345(6202), 1284-1287.
- Ebener, S., et al. (2015). The role of Geographic Information Systems in public health implementation. Global Health Action, 8(1), 29285.
- The Lancet Global Health. (2021). Adaptive management in global health: a necessity, not an option. The Lancet Global Health, 9(8), e1035.