Sustainable Development Goal 7 is one of 17 Sustainable Development Goals established by the United Nations General Assembly in 2015
Overview:
Energy access is essential for proper healthcare service delivery. Healthcare facilities in Nigeria require electricity for lighting, emergency procedures, and storage of vaccines and drugs. Unfortunately, Nigeria’s grid electricity supply has stalled at around 4GW on average and covers only about 57 percent of the population. According to the World Bank, of the 16,900 public healthcare (PHC) facilities in Nigeria, 81 percent lack a reliable power supply. A recent study conducted in the Federal Capital Territory (FCT) shows that power supply to PHCs is intermittent, with an average of 4 hours or less daily. It is worse for facilities not connected to the grid as they rely solely on expensive fossil fuel generators to provide electricity. These generators contribute to both ambient noise and air pollution and are unsuitable for healthcare environments.
Globally, there is a growing interest in alternative power sources, including mini-grids and off-grid solar, which can be highly effective in helping to achieve Sustainable Development Goal 7 (SDG7) by 2030.
The government of Nigeria, other major corporate industry players, and the private sector have worked for years toward realizing the SDG 7. The aim is not just to achieve it but also because lack of or epileptic power supply in public healthcare centers can be life-threatening. Despite the large strides already made, the mini-grid market is yet to reach a tipping point at which it can expand without support. To achieve this, funding is required, but also, getting the right geolocation solution and clean data for informed decision-making remains a challenge.
The Challenge:
Despite the great strides and enormous support made by the government and other stakeholders to ensure that renewable energy is an established, cost-effective alternative source of power in Africa, implementation is still lagging. For example, identifying the right site for a mini-grid may not be easy in Africa because not every region is mapped and assigned a geolocation coordinate. Demography data on residents within some remote and/or security-challenged regions are difficult to find.
A report by the African Development Bank on Green Mini-Grids in Sub-Saharan Africa has identified the lack of up-to-date and reliable data as a barrier to the growth of mini-grids in Africa. As businesses become more reliant on data, the importance of data quality has increased. Data analytics are used to help drive business decisions, therefore, it is important that data must be accurate, complete, reliable, relevant, and timely for it to be trusted. Getting a data set that meets these criteria requires an innovative approach that includes diligence, dedication, and quality assurance throughout the collection process.
The Solution:

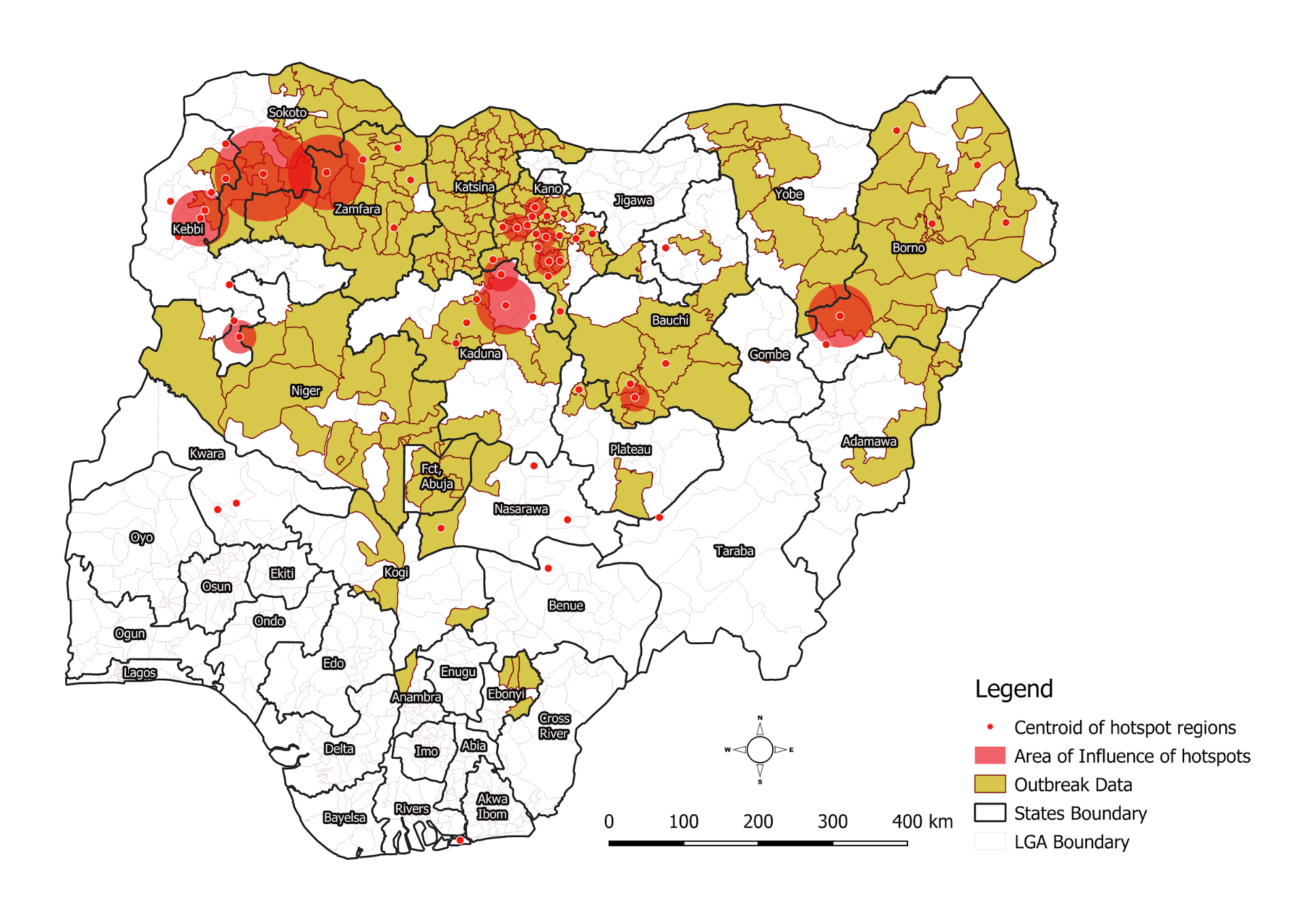
Geospatial intelligence is achieved by visualizing and analyzing geographical data. Organizations can use intelligence tools to identify where an event has taken place, why it is happening, and what caused it by adding layers of geographical information, such as demographics, traffic, and weather data, to smart maps and dashboards. “It’s one of the hottest technologies out there,” said Professor Sunil Bhaskaran, founding director of the Geospatial Center of the CUNY CREST Institute (BGCCCI) at Bronx Community College.
A geospatial platform created by eHealth Africa is The Data Portal. A result of several years of geospatial data collection across Nigeria and some parts of Africa. It contains up-to-date data on points of interest, including schools, settlements, health facilities, and roads, including their population estimates.
The goal of the data portal is to make existing geospatial data accessible and reusable. This will allow organizations to focus resources on programmatic data rather than base geospatial data for their planning and monitoring across Nigeria. A GIS expert with eHealth Africa, Fashoto Oluwatosin Busayo, spoke on the effectiveness of the data portal, “geospatial intelligence is proving to be a more effective way of allocating energy resources than traditional methods. Using this method, it is possible to identify areas that lack access to energy or are underserved. eHealth Africa has provided training on map production and micro-planning with geospatial data freely available on its data portal to various stakeholders” he said.
eHealth Africa’s recent project on Remote Assessment of Energy Gaps in Selected Health Facilities, used the remote survey method of data collection to get accurate, reliable data from 291 health facilities in Kano and Osun states, and 300 health facilities in Nasarawa State. “We deployed this method because it is reliable in security-challenged environments like Nigeria. It is also less expensive. Trained helpdesk agents conducted the remote surveys at eHealth Africa.” said the project manager Mohammed Bello.
eHealth Africa is committed to the design and implementation of innovative data-driven solutions for public health interventions across Africa.